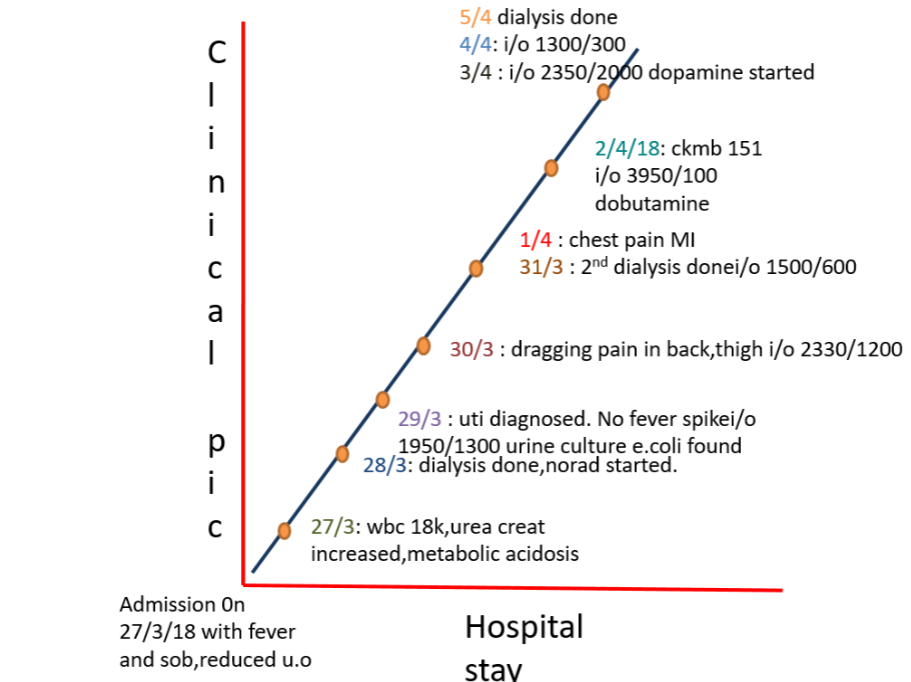
After dinner on my night duty, I rushed to casualty as a patient was brought who needed immediate attention. On going to casualty, I saw that a 60 year old lady was struggling to breathe and appeared tachypnic. Her % oxygen saturation was only 86% at room air. We had to provide her immediate oxygen support which improved her saturation but she was still tachypnic, and opening her mouth to take in the air, basically struggling to take the air in.
After making sure that her saturation was well maintaining I had called the attender to take a detailed history. Her complaints were not of recent onset. She had complaints since the past 4 months. The lady had been having complaints of burning micturition since 4 months. She had been visiting the hospital often for the above complaints. This time, she had the same complaints of burning micturition, fever, abdominal pain and decreased urine output. (figure 1)
 |
| Figure 1 |
On asking further the attenders had told that she hadn't passed the urine since 3-4 days. So I had immediately asked for a Foley's catheterization. The moment we had inserted the Foley's the urine was milky white for the initial few minutes. By this time we had got a few of their old prescriptions which showed a urology op card and the urologist made a diagnosis based upon the history of “thin stream of urine” as stricture urethra. Now everything was falling into place. Her persistent complaints from the past few months, her burning micturition, fever..
 |
| Figure 6 |
Her first visit was in December last year. (figure 7) She had first gone to a gynecologist with complaints of burning micturition, whitish discharge per vagina and fever. Probably the gynecologist had asked her to void and come as they wanted to examine her per vaginally. But this is where we lost her progress. She then landed up in urology OPD where her op card revealed that she had a thin stream of urine. (figure 8) The diagnosis of stricture urethra was made solely based on this and a dilatation procedure was done, she was catheterized with Foley's and urine culture sensitivity was sent. She was started on antibiotic and asked to turn up after 3 days which she did. (figure 9) She got her Foley's removed and was prescribed the 1st line antibiotic for UTI. (figure 10) The urine culture report was unseen, Unseen by the care provider, unasked by the patients. (figure 11) Had the care provider seen the report the scenario today would have been a different one probably. This old couple wouldn't have been probably undergoing all the treatment which they have undergone.
She was asked to follow up after a stipulated time when she never turned up. This again is the scenario of many of our rural patients who treat themselves based on their subjective feeling. Subsequently We got our hands on another op card of January, one month later which again asked for a urine culture sensitivity. (figure 12, 13) Which again was sent but unseen unfortunately. She was prescribed the same 1st line antibiotic as in the first visit. (figure 14) She was then asymptomatic for the next 2 months. When she developed the symptoms she turned up in the casualty in the current state.
 |
| Figure 12 |
 |
| Figure 13 |
 |
| Figure 14 |
The organism was the same since the first report, but sadly the culture reports being unseen she was getting the antibiotic for which the organism was never sensitive. The organism had been evolving since then into a more virulent one.
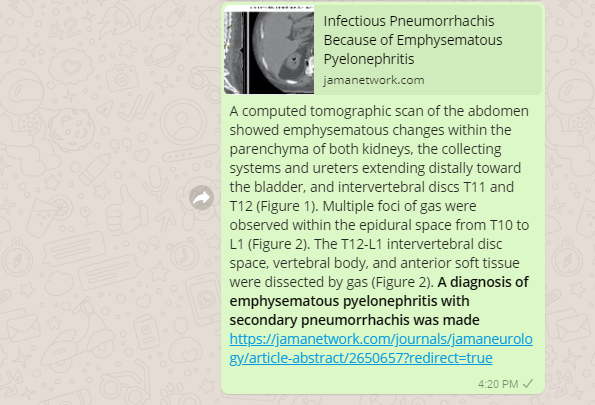
We got a ct abdomen done for her as the ultrasound abdomen revealed pyonephrosis. We had something very unusual and unexpected in store for us in the CT (figure 15,16,17,). She had air pockets in the kidney, in the erector spinae muscle and spinal canal. We decided to change the antibiotic. We were still waiting for the culture report and had started her on a higher antibiotic. But to our dismay our microbiology department didn't have the sensitivity checking disc for the antibiotic which we had started her on.
 |
| Figure 15 |
 |
| Figure 16 |
 |
| Figure 17 |
The old lady was again taken up for dialysis. Unfortunately we had still put her on ionotropic support because her BP wouldn't maintain without it. We had an idea about reaching tachyphylaxis but we couldn't afford to stop the ionotropic support. We continued it further. The lady had been complaining of aching pain in the back, which we attributed it to the continuous lying down on the bed. Now that her leukocyte counts were decreasing (figure 18, 19) and she was maintaining fairly enough on the ionotropic we thought we could pull her back.
 |
| Figure 18 |
 |
| Figure 19 |
In the midnight I get a call on my phone, it was the ICU pg on duty, my Friend who had called me stating that the patient had a MI. They could see few changes in the ecg suggestive of MI.(figure 20) My eyes opened up completely, I was completely awake from my sleep now when she explained the situation. I had asked her to keep monitoring her ecg and to give her the loading doses of anti-platelets and statins. I rushed the next day to the ICU to see the old man standing beside his wife with half tears in his eyes. We hadn't explained him about the MI yet. I didn't have the courage to disclose the fact to him but he had to know. It was much more easier than I had expected. He left to the visitors lounge. He later turned up again after few hours and spoke to me. He started crying. She was the support to him and it was the same with her. They both were each other's strength. He didn't want to loose her and pleaded us to do our best to save her. We assured him that we were trying our best.
 |
| Figure 20 |
The next day ECG (21, 22, 23, 24) interestingly showed an improvement which was unusual. (figure 25) But we were though very cautious about the next development. The lady started loosing her sensorium, the old man started loosing his hope. He would just come see her and go, he was not interested in talking to us. That is probably because we never gave him any positive outcome or a positive news regarding her.
 |
| Figure 21 |
 |
| Figure 22 |
The very next day she started throwing seizures. By this time the old man barely would come.He told he could not see her in so much pain, being restrained. We started her on anti-epileptic. I could see the pain the tears in his eyes, his eyes were wanting to ask us questions, about the possibility of her coming back, about the progress. But he never spoke to us. It was always mediated by her brother. I could not understand why he didn't want to speak. Was he fearful of hearing a bad news or was he not happy with our approach and our care.
The very next day she developed an AF, it was because of the ionotropic we had put her on. We were so helpless, we knew the ionotropic would reach a tachyphylaxis, we knew it would cause AF. But we were left with no choice. We didn't want to loose her, I didn't want to see the old man loose his wife. Whom else did he have? No children, relatives wouldn't bother to take care of a old guy. I didn't want him to loose faith in us, to loose faith in medical system. I wanted him to ask questions, to ask about her. Him not asking questions was bothering me more.
This is the irony of life, few people make a hue and cry of their patient not being attended just as he had a vomiting few hours later after we left, and few people don't wish to speak or listen to us.
That lady ultimately fought back. The repeat CT abdomen showed no gas. It had vanished. (figure 27)The leukocyte count came back to normal. She came back. She gained her sensorium. We were happy that we could pull her back from the point where we had left everything. But He he still was not the same, he was not completely satisfied, probably because he thought that she was not out completely, or probably because he had a experience of loosing her which he knows is going to be the bitter truth ultimately one day.
 |
| Figure 27 |
Now when I look back I see that we had treated her only for the symptoms which she presented with. We didn't do anything for her. She could have a seizure once she stops the anti-epileptic, she could again develop stricture once the Foley's is removed, she could develop the MI again. If she could develop all these again, then what have we done for her?
Online (dugout)* Team Discussion:
* This is also known as "Case based blended learning ecosystem (CBBLE) decision support system CDSS (through social media)








































Comments
Post a Comment